
This is the second in a series of posts which I have written alongside a module I will be teaching which is intended to help non-sociology students to gain an understanding of the sociology of health and illness. While these posts are primarily intended for that audience and are therefore intentionally introductory there might be something of interest to a more general audience. For that reason I have decided to put them on my blog in amongst more specific and specialist writings.
In my previous post I introduced two fundamental aspects of sociological investigation which make it useful for understanding health. These are sociology’s capacity to investigate social structures and experiences, identities and meanings. In this post I will explore social structures and their relationship to health in more detail.
In order to gain a basic understanding of social structures we can suggest that they are:
- Social (not natural)
- “Made up” by human beings
- Constrain and enable human behaviour
- Exist independently of individuals
- Dynamic (change over time)
In the previous post in this series I used the law as an example of a social structure. Fundamentally social structures are exactly what they sound like; the ways in which society is structured. One type of structuring of society which sociologists discuss is social solidarity or a sense of “togetherness”. When investigating social solidarity sociologists investigate the ways in which people are bound together as part of a community (this could be as a nation, city, religious group, family, school, etc.).
One of the earliest sociologists Émile Durkheim investigated the ways in which social solidarity (an aspect of the social structure) had an impact on rates of suicide (what appears to be a very individual behaviour). In a nutshell he found that in societies with higher levels of social solidarity (a greater sense of community) there were lower rates of suicide. So, he concluded that social solidarity was a form of protection against the drive to commit suicide.
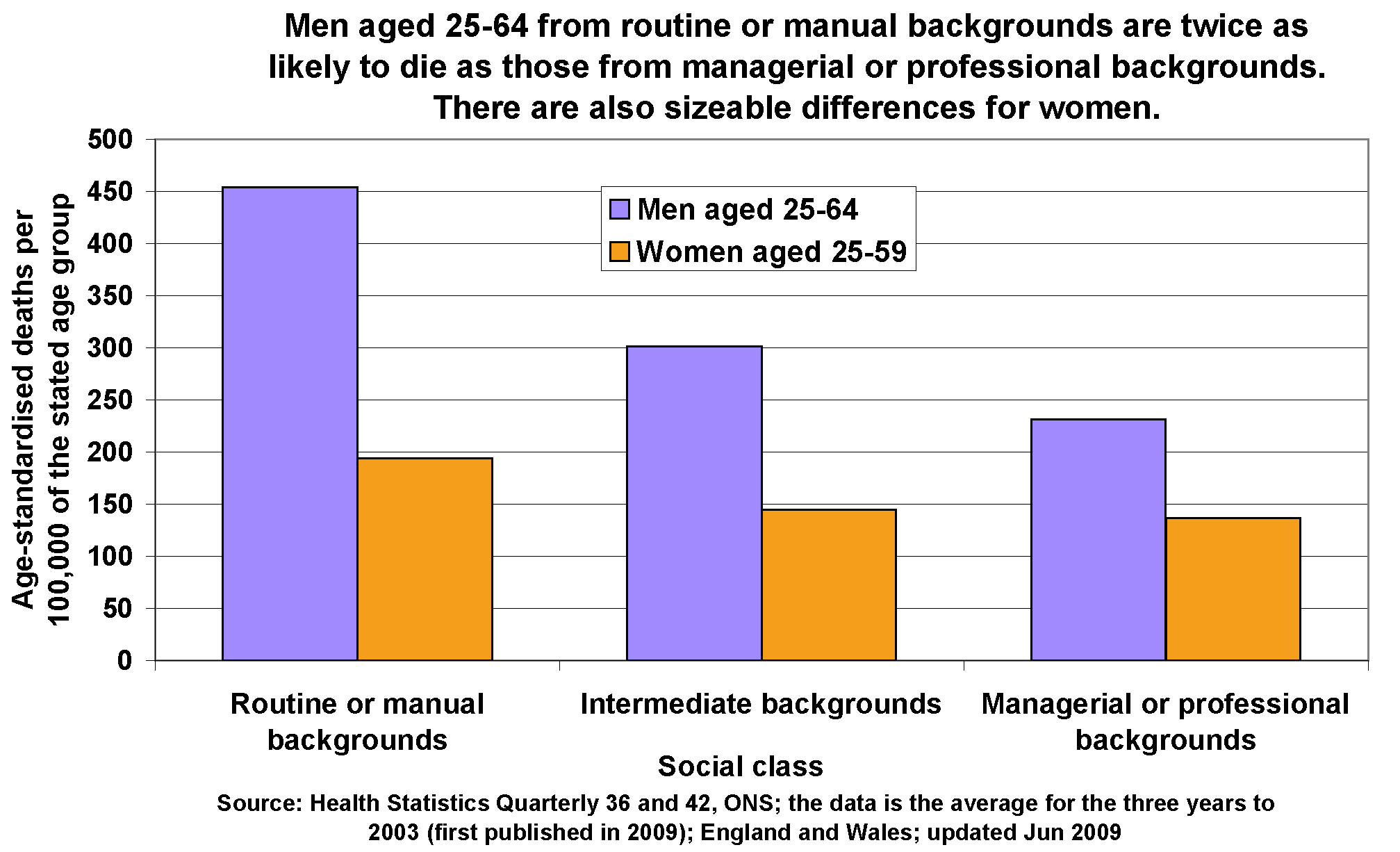
The important thing for our purposes is not his findings as such but the relationship which sociological analysis enables us to draw between social structures and individual behaviours and how this can be applied to health and illness. So, we can look at how rates of premature death are distributed across social class in England and Wales in the bar chart below.
http://www.poverty.org.uk/60/index.shtml
The significant differences in rates of premature death we can see above (you are much more likely to die prematurely if you are a man from a “Routine or manual” rather than “Managerial or professional” background) suggest that social structures (not just individual choices) play some role in health outcomes. If the likelihood of a particular individual dying prematurely was solely due to biology or personal choices then there would not be any particular social patterning. So, we can suggest that there is something in the ways in which society is structured which leads to premature death.
Remember these are structural factors so they are things which “exist independently of individuals” but “constrain and enable” their behaviour. These factors could include:
- Work conditions
- Money for healthy food or exercise
- Access to healthcare
- Motivation to take preventative action
- Housing standards
- Knowledge of, and access to, health strategies
Perhaps the most important thing to remember about these social structural factors is that they are “social (not natural)”, ““made up” by human beings” and “dynamic (change over time)”. So these structural factors can be changed and therefore the health outcomes of particular individuals can be different.
In the next post in this series I will address the relationship between capitalism and health.
